Charting Progress, Changing Outcomes: A New Era of Multiple Myeloma Care

Multiple myeloma (MM) has historically been associated with poor outcomes and limited treatment options.¹ Dr. Xavier LeLeu, Head of the Myeloma Clinic and the Department of Hematology at Hôpital La Mileterie, Poitiers, France, and Zandra Klippel, Head of Oncology Development at Sanofi, are recognized leaders in multiple myeloma, with extensive experience shaping the research and development of therapies across the disease's evolution and know all too well the realities MM patients face.
In many ways, MM was a different disease all together,” said Dr. Leleu. ”There were a few therapeutic options that emerged around the 80s and 90s, but generally speaking treatment failure was common, disease progression was rapid, and there were few avenues clinicians could take when a person inevitably relapsed.

Dr. Xavier LeLeu
Head of the Myeloma Clinic and the Department of Hematology at Hôpital La Mileterie, Poitiers, France
Dr. Klippel added: "The therapeutic options available at the time were limited and often inadequate to achieve sustained disease control in MM."
The MM treatment landscape has changed substantially over the past 20 years driven by the availability of a broader range of therapeutic options that allow for longer disease control.² As a result, median overall survival has increased by up to 50% since the early 2000s, reflecting the measurable impact of these advancements on patient outcomes.³
Despite the progress, the unmet need remains and MM care is still evolving.
The Evolving Multiple Myeloma Treatment Landscape
It's easy to wonder what the turning point was in MM research that charted the course towards the improvements that exist today. But, as Dr. Klippel noted, "it would be nearly impossible to pick just one." Identifying a single turning point in the evolution of treatment is difficult.
Between 2003 and 2023, the research and treatment landscape advanced substantially, with the introduction of more than 15 new therapies.¹ These included targeted agents designed to act on specific molecular pathways implicated in MM, followed by newer approaches that leverage immune‑based mechanisms of action (treatments that help your own immune system fight cancer).⁴ Together, these developments expanded treatment options and progressively reshaped standards of care across different stages of the disease.¹
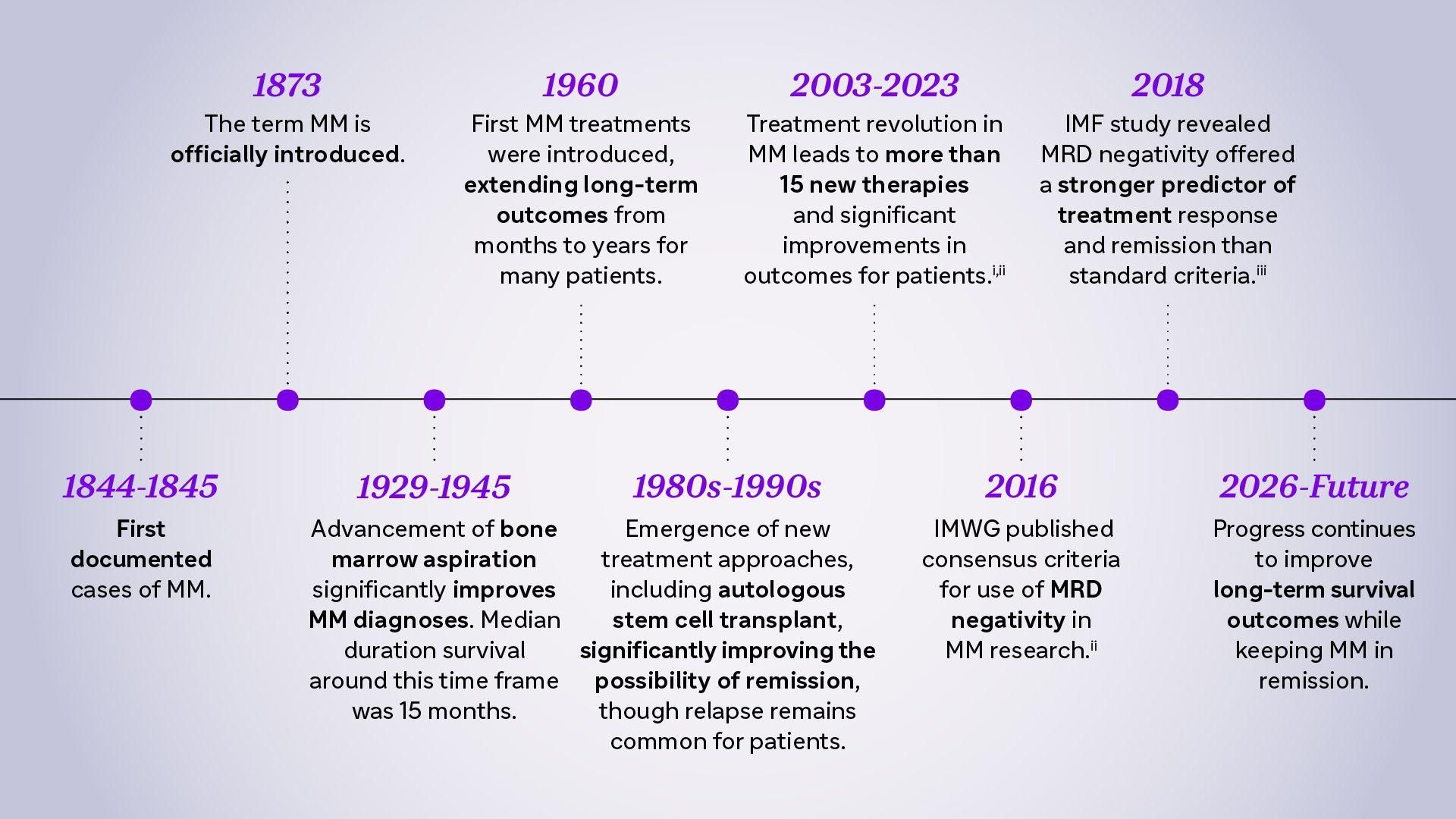
MM research has advanced leaps and bounds since its discovery in the 1800s, improving outcomes for patients throughout the years
Beyond the expansion of available therapies, the emergence and development of tolerable combination treatments marked a shift in the care continuum,⁵ "As understanding of the disease evolved, treatment approaches moved from single agents to combination therapies with complementary mechanisms of action, aiming to generate stronger anti-cancer responses than single agent therapies," said Dr. Leleu. "Today, combination therapies are widely used across all treatment settings."
Setting New Benchmarks for Treatment
Research in MM continues, extending beyond novel therapies. The field has also focused on addressing long-standing hurdles related to treatment response, disease resistance, and long-term patient outcomes.
One of the most common causes of relapse is the presence of residual MM cells after treatment. Even after initial therapy where a patient could go into remission, small numbers of myeloma cells can persist undetected by conventional methods, and may ultimately contribute to disease relapse.⁶
Novel treatments have allowed for more common and deeper responses including complete responses. While we celebrate better long-term outcomes in this infrequent cancer, this success increased the hurdle for bringing new treatment options. The MM community recognized that identifying a reliable early marker for efficacy strongly correlated with long term outcomes would be key to maintaining the pace of innovation in this space.
To address this challenge, researchers have increasingly focused on Minimal Residual Disease (MRD). MRD is a measure of malignant or cancerous cells in the bone marrow following treatment, and represents the deepest measurable level of response. When highly sensitive testing fails to detect residual myeloma cells, this means a patient is considered to have achieved MRD negativity. Numerous independent studies have shown a correlation between MRD negativity and improved long-term outcomes in MM, including longer remission and overall survival rates.⁷
Although MRD has been recognized as a concept for many years, it wasn't commonly incorporated into MM research until the mid-late 2010s. During that time, the International Myeloma Working Group (IMWG) published consensus criteria supporting the use of MRD negativity in MM clinical research, and a later International Myeloma Foundation study validated MRD negativity as a strong predictor and endpoint of MM treatment response and remission.⁸'⁹
When I was practicing, MRD negativity was a known concept, but it wasn’t something we were actively measuring in research, let alone clinical practice. Now, MRD negativity is a mainstay in MM clinical trials, and we’re even evaluating sustained MRD negativity to better understand if we are able to stop treatment without affecting long-term outcomes.

Dr. Zandra Klippel
Sanofi's Head of Oncology Development and former clinician
MRD negativity is becoming an increasingly important treatment goal across the entire MM care continuum, but it’s particularly important for patients who are newly diagnosed. “In newly diagnosed multiple myeloma, the first-line therapy is critical because it could impact the long-term course of the disease,” said Dr. Leleu. “That’s why MRD negativity is increasingly used as an important endpoint. It helps us understand how deeply patients are responding during early treatment and could support further and future efforts to achieve longer-lasting disease control.”
The Next Era in Multiple Myeloma Care
Advancements in MM research have had a lasting impact of helping to extend patient lives. While there is still no cure, many patients can now manage their disease for longer than before. However, the ongoing burden of treatment can still affect quality of life.
For instance, we’ve made a point to design clinical trials that look at both clinical and health-related quality-of-life endpoints, to ensure patients’ broader physical, mental and emotional health are taken into consideration when evaluating new treatments.
We’re also exploring new ways to address common challenges in MM treatment administration, including lengthy infusion times. By pursuing innovation in subcutaneous treatment delivery, we are exploring approaches that may address some of the complexities that impact the patient treatment experience.
“We are honored to have been part of the broader MM community all these years and hope to continue drive research towards better outcomes for people affected by MM across the disease continuum,” said Dr. Klippel.
Broadly, the MM research community is always striving for better, and the field continues to progress with urgency to further improve outcomes and extend lives. While there is much work yet ahead, it’s also important to acknowledge the progress that has been made to date.
“In Myeloma, improving survival has long been the primary objective, and for good reason,” said Dr. Leleu. “As we continue to look for ways to continue to extend survival outcomes, working toward a potential cure represents a key area of research. But survival is only half the battle. True innovation must focus on improving the entire treatment journey for patients, families and caregivers alike.”
Explore More
MMoving Forward: Sparking Change in Multiple Myeloma
Addressing Unmet Needs in Multiple Myeloma Research
Adjusting to Life with Multiple Myeloma: Bernard’s Story
References
- Elbezanti WO, Challagundla KB, Jonnalagadda SC, Budak-Alpdogan T, Pandey MK. Past, Present, and a Glance into the Future of Multiple Myeloma Treatment. Pharmaceuticals. 2023;16(3):415. doi:https://doi.org/10.3390/ph16030415
- Mo CC, Hartley-Brown MA, Midha S, Richardson PG. Upfront or Deferred Autologous Stem Cell Transplantation for Newly Diagnosed Multiple Myeloma in the Era of Triplet and Quadruplet Induction and Minimal Residual Disease/Risk-Adapted Therapy. Cancers. 2023;15(24):5709. doi:https://doi.org/10.3390/cancers15245709
- Dores GM, Vo JB, Schonfeld SJ, et al. Temporal patterns in US population-based patient survival among adults treated with chemotherapy and/or immunotherapy for multiple myeloma, 2000-2020. British journal of haematology. Published online October 2025:10.1111/bjh.20192. doi:https://doi.org/10.1111/bjh.20192
- Mayo Clinic. Multiple myeloma - Diagnosis and treatment - Mayo Clinic. Mayoclinic.org. Published 2019. https://www.mayoclinic.org/diseases-conditions/multiple-myeloma/diagnosis-treatment/drc-20353383
- Mokhtari RB, Homayouni TS, Baluch N, et al. Combination Therapy in Combating Cancer. Oncotarget. 2017;8(23). doi:https://doi.org/10.18632/oncotarget.16723
- Watson S. What to Know About Relapsed Multiple Myeloma. Healthline. Published October 2, 2023. Accessed May 15, 2026. https://www.healthline.com/health/multiple-myeloma/what-to-know-about-relapsed-multiple-myeloma
- Kumar, S., Paiva, B., Anderson, K. C., Durie, B., Landgren, O., Moreau, P., Munshi, N., Lonial, S., Bladé, J., Mateos, M. V., Dimopoulos, M., Kastritis, E., Boccadoro, M., Orlowski, R., Goldschmidt, H., Spencer, A., Hou, J., Chng, W. J., Usmani, S. Z., Zamagni, E., … Avet-Loiseau, H. (2016). International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. The Lancet. Oncology, 17(8), e328–e346. https://doi.org/10.1016/S1470-2045(16)30206-6
- Cavo, M., San-Miguel, J., Usmani, S. Z., Weisel, K., Dimopoulos, M. A., Avet-Loiseau, H., Paiva, B., Bahlis, N. J., Plesner, T., Hungria, V., Moreau, P., Mateos, M. V., Perrot, A., Iida, S., Facon, T., Kumar, S., van de Donk, N. W. C. J., Sonneveld, P., Spencer, A., Krevvata, M., … Munshi, N. (2022). Prognostic value of minimal residual disease negativity in myeloma: combined analysis of POLLUX, CASTOR, ALCYONE, and MAIA. Blood, 139(6), 835–844. https://doi.org/10.1182/blood.2021011101